One of the most common frustrations expressed by restorative dentists involves the placement and longevity of composite tooth restorations. Tooth restorations, commonly referred to as “dental fillings,” are foundational and arguably the most important treatment in everyday practice. This is especially true in insurance-based practices where reimbursements rates for direct composite procedures are low (and often decreasing) and overhead is a common concern. Adhesive dentistry, however, is highly technique sensitive and should not be rushed, regardless of current industry trends and messaging touting simplified and faster placement methods.
When done without proper isolation, at high speed, and with simplified materials, composite “fillings” can lead to leakage, recurrent caries, and post-operative sensitivity. These preventable adverse outcomes often decrease patients’ trust and confidence in the dental team. However, when executed meticulously using proper isolation, engineering principles, optimal materials, and sound technique, composite restorations are a long-lasting restorative solution that facilitate the preservation of maximum healthy tooth structure and pulp vitality. This is the number one goal of the Biomimetic dentist.
BIOMIMETIC RESTORATIVE DENTISTRY
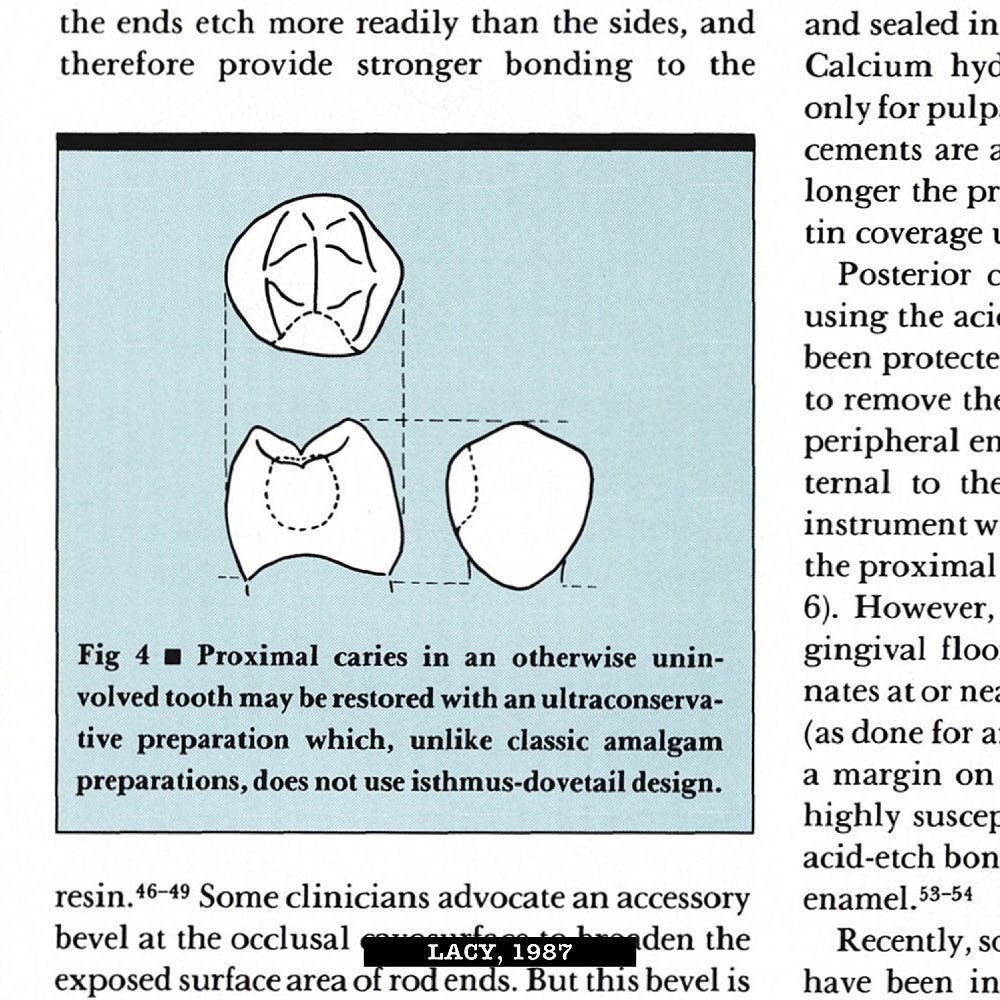
In the amalgam era, a retentive hole was prepared in a tooth and filled with a self-setting alloy. Though unsightly and relatively aggressive in nature, amalgam fillings have saved countless teeth in the Western world for over 150 years. In contrast, modern adhesion with composite resin enables dentists a far more esthetic and conservative treatment approach. But here’s the kicker: adhesive dentistry is far more complex and technique sensitive than amalgam, and clinicians often fail to recognize the differences between the two materials. Most dental schools in the United States still teach antiquated concepts of retention and resistance form which is necessary for amalgam yet often catastrophic for composite.
Short-lived composite restoration with recurrent caries and cuspal fracture on a teenager girl. Plaque disclosing solution applied to the tooth (far left). Defective composite and caries removal followed by air-particle abrasion (middle left). Immediate Dentin Sealing (IDS) and resin coat (middle right). Incremental cusp replacement with final high-shine polish (far right).
With adhesive dentistry the goal is no longer to simply fill a hole but rather connect the composite restoration to the tooth with virtually zero mechanical retention from bottom to top, side to side, and front to back. This is only possible with a firm understanding of and respect for tooth substrate properties, adhesion principles, material properties, isolation techniques, preparation design, and incremental, stress-reducing material placement techniques. Dentists must learn to trust adhesion. By changing the mentality from simply filling a hole to restoring a tooth defect in a manner that mimics the properties and function of a natural tooth, clinicians can create highly bonded, long-lasting tooth restorations.
Welcome to Biomimetic Restorative Dentistry.
IS FASTER ALWAYS BETTER?
In a modern society that has solidified an addiction to the convenience of fast food, deliveries, and travel, the demand for speedy service in all industries is increasing. Of course, the dental team certainly has incentive to work efficiently. This is driven partially by patient demand for shorter visits to minimize discomfort in the dental setting, but can mostly be attributed to industry pressures such as low insurance reimbursement rates and high overhead. Dental material manufacturers understand these challenges and have responded by offering simplified materials promoted with language that encourages faster placement to reduce treatment times.
In adhesive dentistry, however, faster doesn’t always mean better. In fact, rushing adhesive procedures often results in post-operative sensitivity, reduced longevity, and even catastrophic failure, which translates into return visits, zero-production redos, and increased frustration. While there has been impressive advancements in dental materials such as universal adhesives and bulk fill composites, these products have yet to surpass the quality and performance of two-step, gold standard adhesives and incremental placement techniques (Van Meerbeek et al, 2009). Either way, clinical success, independent of material choices, will ultimately be determined by the skill level and technique of the operator.
ABSOLUTE ISOLATION
There are many “isolation” strategies on the market, but no product offers the level of absolute isolation provided by a rubber dam. A properly placed rubber dam provides the operator and patient a clean surgical field free of moisture from breath, sulcular fluids, and saliva while retracting soft tissue and lips for maximum access and efficiency. Eliminating the need for the clinician or assistant to retract the lips or tongue can also help mitigate hand and wrist fatigue. As such, team members welcome and often favor the use of rubber dam in practice.
Though some patients protest rubber dam initially, they often welcome the idea of increased comfort by not having to endure excess water pooling, tooth and material debris, and risk for iatrogenic injury to soft tissues during treatment, in addition to the procedural benefits mentioned above. A clinician that communicates their intentions to patients not only shows they care about the patient’s comfort, but also that they prioritize the quality of their work.
With proper training, rubber dams can be placed efficiently in a matter of minutes by either the doctor and/or assistant. With a rubber dam employed, the clinician can efficiently prepare teeth, spread load the bonding protocol across multiple teeth, and even leave for hygiene checks or other tasks, giving dentin bonds ample time to mature without risk of contamination. Absent the absolute isolation offered by rubber dam, clinicians must battle multiple intra-oral variables that can prove catastrophic for an otherwise sound bonding protocol.

Anterior sextant therapy prior to air-particle abrasion and adhesive application. Sextant or quadrant strategies afford the clinician an opportunity to spread-load the bonding and restorative protocol across multiple teeth, allowing time for hybrid layer development free of competing stresses from composite placement.
TIME IS ON YOUR SIDE
The Biomimetic Restorative Dentist understands the importance of time in adhesive procedures and strategizes accordingly. Time is crucial particularly in dentin-rich scenarios where formation of a high-quality hybrid layer relies heavily on the ability of dentin bonds to fully mature free of stress. Stacking composite in large increments too quickly on a developing hybrid layer causes delamination at the dentin-adhesive interface as shrinkage stresses in the composite exceed the slowly developing dentin bonds (Alleman et al, 2021). This concept is appropriately referred to as the “adhesive equation” and is not unique to dentistry.
For example, the instructions for use for 3M’s Command Picture Hanging Strips advises users to wait 1 hour after application on a surface for the “adhesive to build” before loading. Given time to set, the load-bearing capability of these strips is still dependent on the surface they’re applied to as well as the surface area of the strip. Similarly, the total surface area of each unique tooth substrate, surface treatment of those substrates, and proper application of the adhesive according to the manufacturer's IFU contribute to the overall bond-ability of the tooth.
One misconception about adhesive dentistry is that enamel bonds are stronger than dentin. However, given adequate time and proper isolation, a two-step, gold-standard bonding system such as Kuraray’s SE Bond, SE Bond 2, or SE Protect can produce a bond to dentin up to twice the strength as the bond to enamel (Van Meerbeek et al, 2003). Respecting time requirements for bond maturation, regardless of the bonding system used, helps mitigate leakage, eliminate post-operative sensitivity without the need for additional desensitizing products (Brannstrom, 1986), and enhance bond performance.
Whether you're applying a Command Strip to the wall or bonding a tooth, the common denominator in achieving a successful outcome is time. Understanding how the adhesive equation applies to composite dentistry and altering one’s restorative protocol to accommodate the concept will help improve clinical outcomes, thus increasing doctor and patient satisfaction. Time is on your side - use it where it matters most.

Immediate Dentin Sealing (IDS) with CLEARFIL SE Protect and 0.5mm flowable resin coat with CLEARFIL Majesty Flow prior to matrix assembly. Dentin bond maturation begins at light cure and continues for 10-20 minutes (Sadr et al, 2019). Time required for matrix assembly mitigates stressing the developing hybrid layer too early, creating a secure bond strategy that prevents leakage and post-operative sensitivity (Krejci, 2000).
KEY TAKEAWAYS
There’s a popular military adage known as the 7 Ps used to emphasize the importance of planning to achieve mission success: Proper Planning and Preparation Prevents Piss Poor Performance. Indeed, success relies heavily on meticulous planning supported by reproducible protocols and the mitigation of any condition or risk that could compromise the mission. This is applicable not just in the military but all aspects of life, including in dentistry. Biomimetic Restorative Dentists seek to deliver the highest quality of care in adhesive dentistry through meticulous, evidence-supported, uncompromised restorative protocols.
Despite messaging from some manufacturers that might suggest otherwise, adhesive dentistry is a highly technique sensitive discipline that cannot be executed in a “simple way” (Van Meerbeek et al, 2001). Clinicians throughout the world routinely express frustrations with short- term longevity, staining, and post-operative sensitivity, while humbly seeking solutions to correct and prevent them. For most, the answer to making adhesive dentistry more enjoyable and predictable lies in developing a deeper understanding of dental adhesion, improving surgical field access and management with rubber dam isolation, and slowing down restorative workflows where time matters most.
To learn more about science-driven Biomimetic Restorative Dentistry, visit www.practicalbrd.com.
REFERENCES
Alleman, D.S; Alleman, D.S; Deliperi, S; Aravena Diaz, J; Martins, L; Keulemans, F. Decoupling with time. Inside Dentistry. Aug 2021.
Brannstrom M. The hydrodynamic theory of dentinal pain: sensation in preparations, caries, and the dentinal crack syndrome. J Endod. 1986 Oct;12(10):453-7. doi: 10.1016/ S0099-2399(86)80198-4. PMID: 3465849.
Hayashi J, Espigares J, Takagaki T, Shimada Y, Tagami J, Numata T, Chan D, Sadr A. Real-time in-depth imaging of gap formation in bulk-fill resin composites. Dent Mater. 2019 Apr;35(4):585-596. doi: 10.1016/j.dental.2019.01.020. Epub 2019 Feb 25. PMID: 30819550.
Krejci, Ivo and Minos M Stavridakis. “New perspectives on dentin adhesion--differing methods of bonding.” Practical periodontics and aesthetic dentistry: PPAD 12 8 (2000): 727-32; quiz 734.
Van Meerbeek B, De Munck J, Mattar D, Van Landuyt K, Lambrechts P. Microtensile bond strengths of an etch&rinse and self-etch adhesive to enamel and dentin as a function of surface treatment. Oper Dent. 2003 Sep-Oct;28(5):647-60. PMID: 14531614.
Van Meerbeek, B et al. “Adhesives and cements to promote preservation dentistry.” Operative Dentistry (2001): 119-144.
Van Meerbeek B, Peumans M, Poitevin A, Mine A, Van Ende A, Neves A, De Munck J. Relationship between bond-strength tests and clinical outcomes. Dent Mater. 2010 Feb;26(2):e100-21. doi: 10.1016/j.dental.2009.11.148. Epub 2009 Dec 16. PMID: 20006379.